Recently, a complex liver operation, headed by Khachatur Badalyan Head of the Chair of Surgical Diseases and Modern Surgical Technologies of the National Institute of Health; Surgeon, Oncologist, Doctor of Medical Sciences, Professor was performed at «Izmirlian» Medical Center.
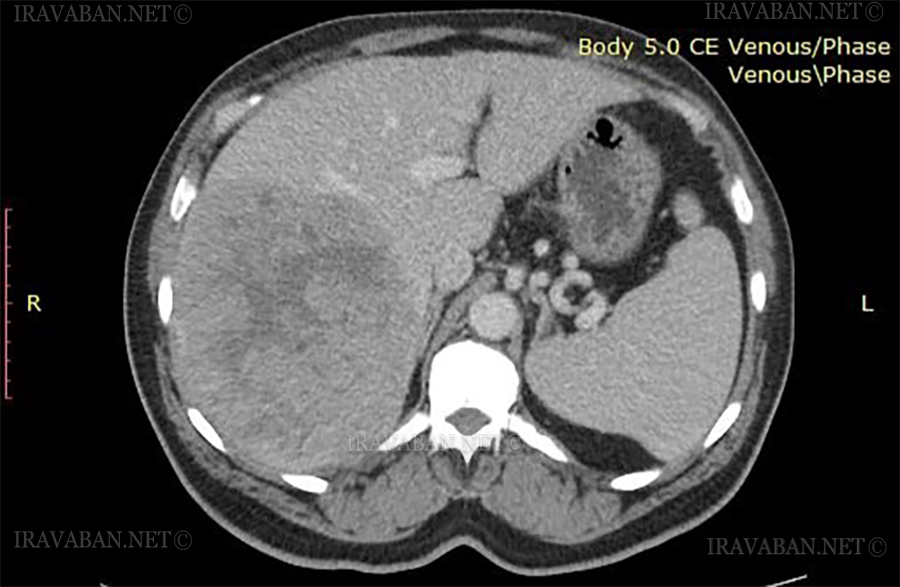
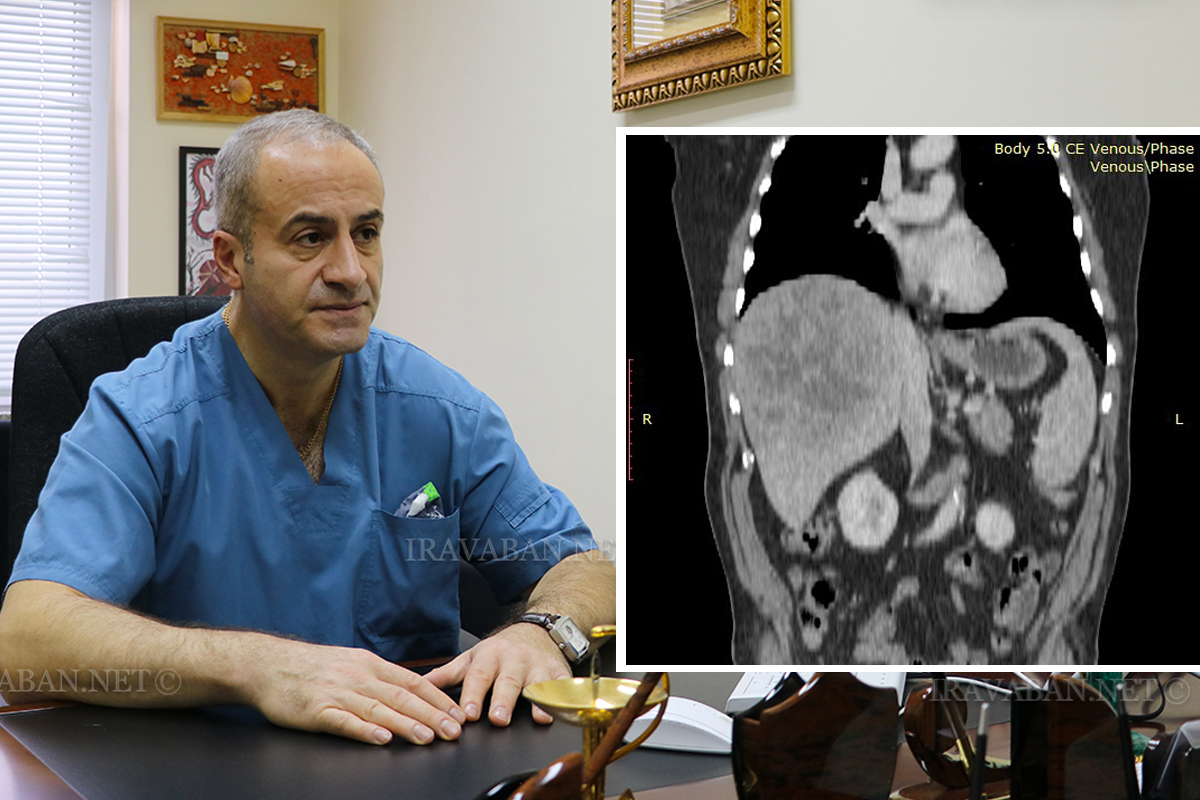
In a conversation with Iravaban․net, Professor Khachatur Badalyan mentioned that we are talking about a tumor center in the liver, which was large in volume and included the hepatic veins and the branches of the vein. The patient had applied to several places, they had refused, saying that it was impossible to remove it.
“There was also an anatomical feature, that is, it was not a pathology, but a feature of vascular anatomy, when in a severe condition, in case of a large tumor, and it makes it technically more difficult to perform surgery. It was a localized tumor, embedded in the diaphragm. It was very difficult, in that large size, about 20-25 cm, the tumor was located under the diaphragm, was located in the direction of the right flexor of the ribs and was inserted into the chest cavity. In other words, inserting a diaphragm into the chest cavity and removing technically similar tumors is often very problematic, because there is some technical support to stop the intraoperative bleeding, or at least reduce it to make the operation real.
 There are problems from the point of view of security, which, unfortunately, does not exist in Armenia, in practice, in any clinic. Given the experience of life and the approaches of technical methodology, that is, how to approach this issue: you know you have to remove it, but how to approach it, so that the intraoperative bleeding is not too much, so that it does not lead to death in the most difficult situation, if the patient loses a large amount of blood. In other words, it is technically necessary to plan this activity in such a way that the amount of intraoperative bleeding is reduced to a maximum,” the doctor says.
There are problems from the point of view of security, which, unfortunately, does not exist in Armenia, in practice, in any clinic. Given the experience of life and the approaches of technical methodology, that is, how to approach this issue: you know you have to remove it, but how to approach it, so that the intraoperative bleeding is not too much, so that it does not lead to death in the most difficult situation, if the patient loses a large amount of blood. In other words, it is technically necessary to plan this activity in such a way that the amount of intraoperative bleeding is reduced to a maximum,” the doctor says.
Khachatur Badalyan mentions that one of the peculiarities of the operation was the planning of the operation, what to do after each step, what complications can occur, how to prevent those complications from occurring, and so on.
According to the doctor, the important fact is that every activity must be licensed and privatized, that is, it should not be a licensing of general oncology, but a separate licensing of liver oncology.
“If a person goes to a clinic and they say no, it is impossible to do, he goes home and says it is impossible to do it and that is all. But if a person applies to a clinic licensed for liver treatment, a full-fledged professional approach is needed. And in that situation, if it is possible to do something, it is necessary to do the maximum. If a person is not able to go abroad, where they have the equipment or specialists, they can perform the operation, most of the clinics refuse, they are afraid of losing the person and that is it,” the professor notes.
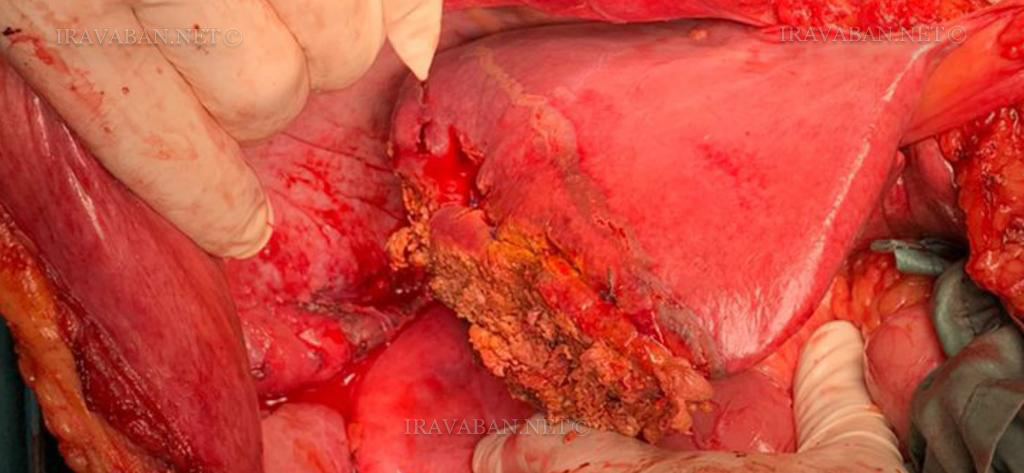
This operation lasted 9 hours, 60% of the liver was removed, because the tumor in the patient had doubled the size of the liver.
“During those 9 hours, there was a very tense situation and it was physically very difficult to perform that operation. There was no replacement. Specialists must have a replacement, when a group works for a few hours abroad, they are replaced by another brigade. OK, I leave it and go out, should nothing be done for the patient? But I am also a human being, maybe I get sick, maybe I feel bad ․․․ In that case, you cannot provide the person with the maximum medical care he needs.
There is no talk about the lack of medical education now, most of the doctors are afraid to teach, not to make them competitors for themselves. This is painful. That is why I want and it is my dream to do that, to teach these specialists so that I can be proud of them, save people’s lives. We should not think about having competing specialists, but about the future of the people, what can be done to continue that work. My residents have probably seen more in the last year than many experienced doctors,” Khachatur Badalyan said.
The professor mentioned that the loss of intraoperative blood was about one liter, and for such surgeries 2-3 liters at the time, when it was done in Moscow, was considered a standard amount․ “It is such a difficult operation that it was a norm and we have developed a method on how to reduce blood loss.”
The patient is feeling well and is now undergoing general treatment.